Naso-temporal
Asymmetry of OKN (Motion Perception) / Reversing Grating Test
Ai-Hou Wang, M.D., Ph.D.
Monocular
optokinetic nystagmus (OKN) in infants and young children is nasal-temporally
asymmetric. Images moving from temporal to nasal side induce a temporal beating
nystagmus; however, images moving from nasal to temporal side do not induce a
nasal beating nystagmus. In other words, the right eye prefers leftward-moving
images, producing a rightward-beating nystagmus, but not a leftward-beating
nystagmus for rightward-moving images. The left eye, in contrast, prefers
rightward-moving images, producing a leftward-beating nystagmus, but not a
rightward-beating nystagmus for leftward-moving images.
The
right eye prefers leftward-moving images.

The
left eye prefers scenes moving to the right

In
individuals without strabismus, this nasal-temporal asymmetry gradually
develops into nasal-temporal symmetric OKN between three and seven or eight
months of age. In patients with congenital esotropia, this nasal-temporal
asymmetry persists and does not develop into nasal-temporal symmetry.
This
preference for the temporal beating nystagmus is identical with the direction
of latent nystagmus (LN), a characteristic of early-onset strabismus.
Furthermore, the timeline for the OKN development from nasal-temporal asymmetry
into symmetry coincides with the development of stereopsis. Furthermore, OKN is
also nasal-temporal asymmetric in animals with bilaterally positioned eyes that
lack binocular vision. All of this suggests a close correlation between
nasal-temporal symmetry in OKN and binocular vision. Tychsen L of the
University of Washington has provided a detailed explanation in the binocular
vision chapter of previous editions of Adler’s physiology of the eye.
Tychsen
L. Binocular vision. In: Hart WM, editor. Adler's Physiology of the Eye:
Clinical Applications, 9th ed. St. Louis: Mosby; 1992: 773–853.
Nasal-temporal
asymmetry of OKN is a characteristic sign of early-onset strabismus. In
patients with anisometropic amblyopia, even if one eye has severe amblyopia and
lacks stereopsis, OKN is still nasal-temporal symmetric. Nasal-temporal
symmetry of OKN can therefore help differentiate between strabismic amblyopia
and anisometropic amblyopia.
We
developed a Reversing Grating Test on personal computer screen to test the
nasal-temporal symmetry of OKN.
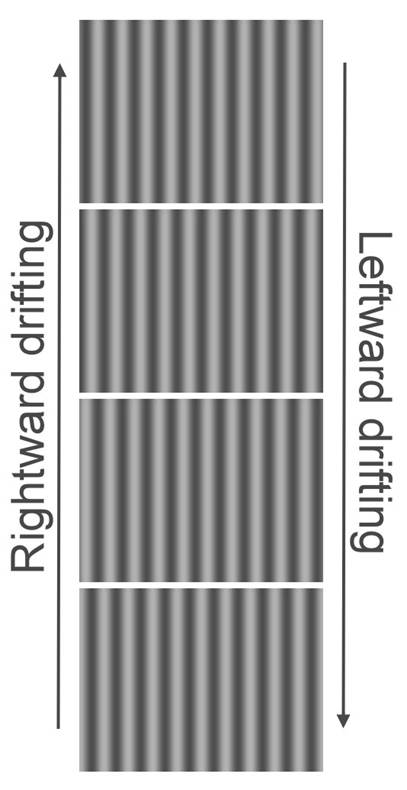
On a
computer, the moving stripe pattern used in OKN testing involves looping four
stripe patterns with 90° phase shifts (see image). If played from top to
bottom, the stripes move to the left; if played from bottom to top, they move
to the right.
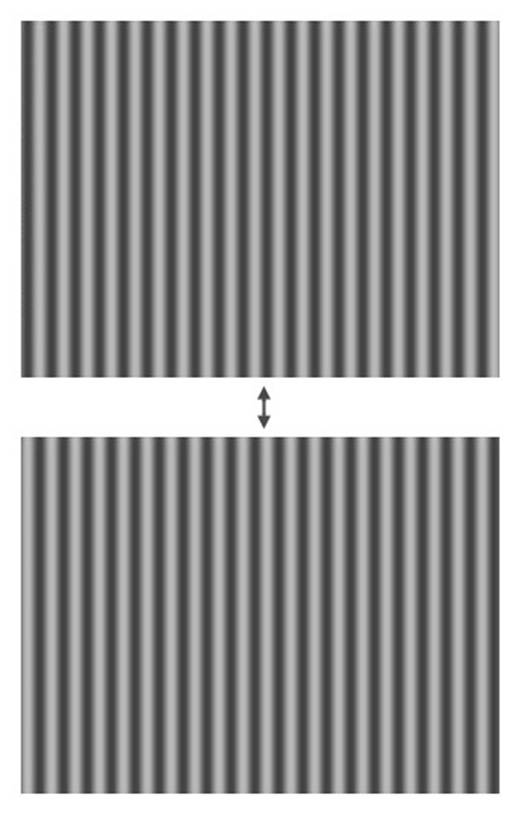
Reversing
grating is a dynamic grating, played back and forth repeatedly between two
grating patterns of opposite black and white colors. Unlike OKN, where four
grating patterns 90° out of phase are played consecutively, reversing gratings
can be thought of as two grating patterns 180° out of phase played back and
forth repeatedly (see image).
Each
reversal can be viewed as a stripe-width moving either to the right or to the
left. The dynamic image of reversing grating is physically left and right
symmetrical, or in other words, the weight of leftward and rightward movements
is equal. When the reversing grating is played to a normal person with
symmetrical nasal/temporal OKN, it appears as flickering stripes. However, when
viewed by individuals of asymmetric nasal-temporal OKN, it appears similar to
OKN stripes moving to the left when viewed with right eye, while appears as OKN
stripes moving to the right when viewed with left eye. And at the same time OKN
will be evoked.
It is
the same image of a reversing grating, when viewed with the right eye, it
produces a rightward beating nystagmus; when viewed with the left eye, produces
a leftward beating nystagmus – identical with the direction of latent
nystagmus!
The
moving stripes of OKN can be physically described by a wave equation of
brightness, while the reversing grating can be described as a standing wave.
The reversing grating can be thought of as the sum of two wave equations of
identical wavelength, one moving to the left and one moving to the right, with
the same speed (see figure).


Reversing Grating OKN
to L OKN
to R
If a
normal person with symmetrical nasal-temporal OKN looks at a reversal grating
without moving his/her eyes, they see flickering stripes. However, if he/she
gazes following a pen tip that moves left and right across the screen, he/she
will see leftward-moving stripes when gazing leftward, and see rightward-moving
stripes when gazing rightward.
Since
a reversing grating can be viewed as the sum of equal weighted rightward moving
OKN stripe and leftward moving OKN stripe, a leftward shifting gaze increases
the weight of the leftward-moving stripe in the sum, resulting in the
perception of a leftward-moving OKN stripe. Conversely, a rightward shifting
gaze increases the weight of the rightward-moving stripe in the sum, resulting
in the perception of a rightward-moving OKN stripe.

Look
at the moving red dot over the reversing grating.
When
the dot goes leftward the stripes look like leftward moving OKN stripes;
when
the dot goes rightward the stripes look like rightward moving OKN stripes.
Individuals
with nasal-temporal asymmetry of OKN have a physiological preference for
leftward-moving stripes in the right eye and rightward-moving stripes in the
left eye. Without external induction of leftward or rightward gaze shifts, the
right eye naturally perceives a reversing grating as a leftward-moving stripe,
which induces leftward pursuit. The leftward gaze shift mentioned above then
increases the weight of the leftward-moving stripe within the total reversing
grating, further strengthening the tendency to perceive the reversing grating
as leftward-moving. This creates a positive feedback loop, amplifying the
latent nystagmus that typically occurs only when one eye is covered, in
early-onset strabismus. Viewing the same reversing grating, right eye viewing
manifests rightward beating nystagmus, while left eye viewing manifests
leftward beating nystagmus. Clinically, reversing grating test can be used to
diagnose the early-onset nature of strabismus.
Interestingly,
the reversing grating test, or the test for nasal-temporal symmetry in OKN, is primarily
a monocular test, but its interpretation is often associated with binocular
vision. A person with esotropia cannot fuse and does not pass stereopsis tests
even after surgical correction to beautiful alignment, reversing grating test
can be performed on either single eye. If the OKN is symmetrical
nasal-temporally, it suggests late-onset strabismus, and stereopsis may be
possible to recover later-on. If the OKN is asymmetrical nasal-temporally, it
suggests early-onset strabismus, and stereopsis is unlikely to be restored.
For
infantile esotropia (congenital esotropia), the general consensus is to correct
the eye alignment surgically before the age of two years. More proactive
physicians may even perform surgery as early as four months of age. The goal of
early surgery is to remove binocular suppression and restore binocular vision.
But what aspects of binocular vision are being restored?
(1) Random-dot stereopsis
seems impossible to recover;
(2) Peripheral fusion in
monofixation syndrome may be restored;
(3) Jampolsky A, Norcia AM,
and Tychsen L tested the symmetry of nasal-temporalward motion perception with
visual evoked potential (VEP) and found that it can be restored through early
surgery.
Norcia AM, Hamer RD, Jampolsky A, Orel-Bixler D. Plasticity
of human motion processing mechanisms following surgery for infantile
esotropia. Vision Res. 1995 Dec;35(23-24):3279-96.
Tychsen L, Wong AMF, Foeller P, Bradley D. Early Versus
Delayed Repair of Infantile Strabismus in Macaque Monkeys: II. Effects on
Motion Visually Evoked Responses. Invest Ophthal & Vis Sci March 2004,
Vol.45, 821-827.